Edwards Syndrome: Symptoms and Causes

Genetic alterations are characterized by being unpredictable and, in many cases, can make life nearly impossible. In today’s article, we’ll look at one such condition, Edwards syndrome, also known as trisomy 18
This pathology owes its name to the man who first described its condition: John Edwards. Unfortunately, it’s a rather serious disease that often causes multiple malformations.
What is Edwards syndrome?
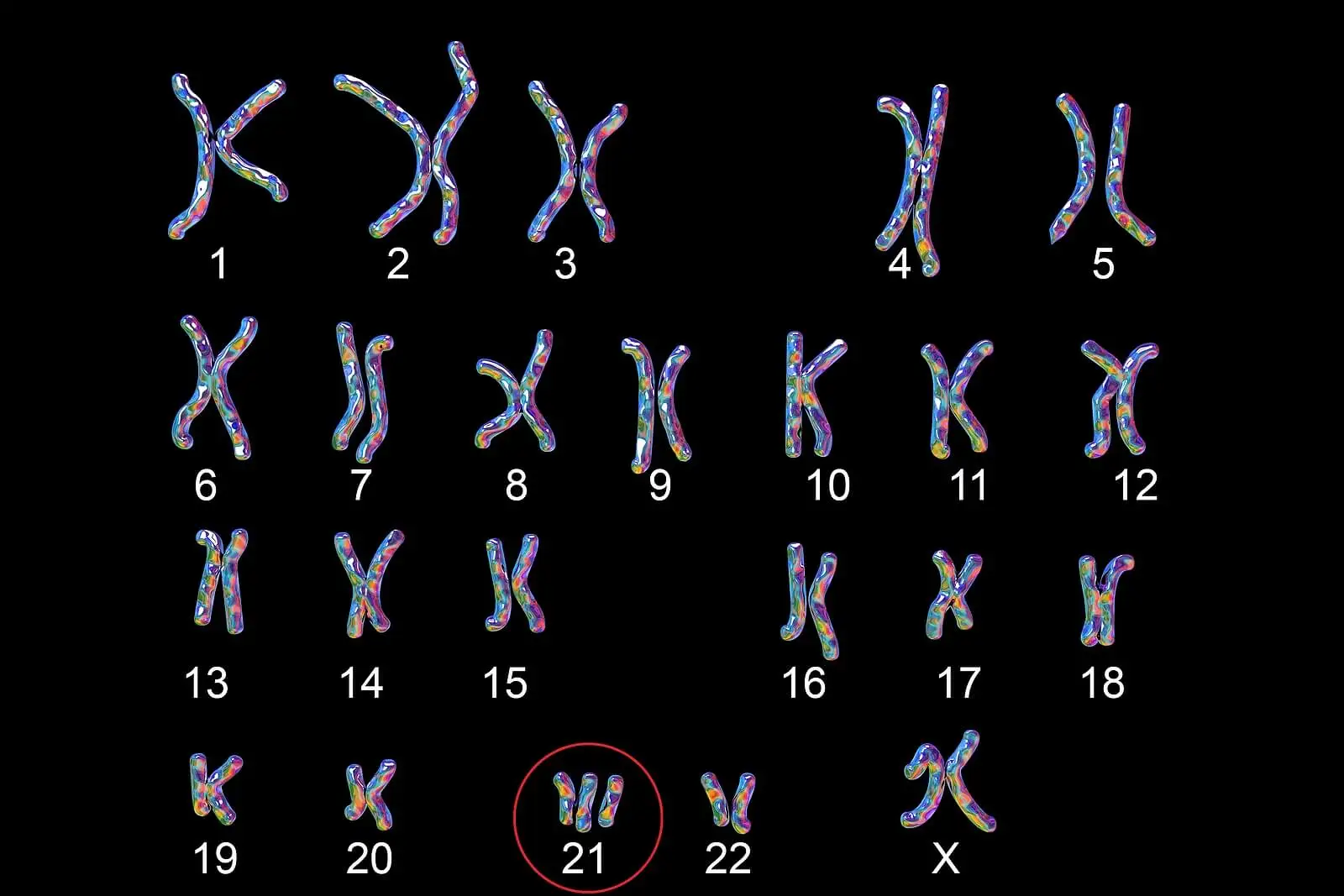
Edwards syndrome is a genetic disease also known as trisomy 18. This means that the baby will have an extra chromosome 18. Because of this, its genetic load will be 47 XX or 47 XY, depending on the sex.
Fortunately, it’s a non-heritable condition, so it can’t be transmitted from parents to children. Its occurrence is only related to abnormalities during gametocyte formation.
It can occur in 1 in 6000 live births, making it the second most common genetic disease, according to records. In addition, it’s a much more common condition in girls, with a ratio of 3 to 1 in girls to boys.
Read also: The Genetic Origin of Sex: the X and Y Sex Chromosomes
Symptoms
Edwards syndrome is characterized by multiple malformations in children, which are present from birth. However, not all symptoms appear simultaneously.
Among the most common clinical manifestations are the following:
- Psychomotor retardation
- Low-set ears
- Small head and jaw
- Constant clenched fists
- Prenatal growth retardation
- Permanently crossed legs
- Underdeveloped fingernails and toenails
- Prominent heel and feet turned inward
- A low birth weight averaging approximately 2,300 grams
Most children affected with Edwards syndrome have some form of congenital heart disease. Cardiovascular abnormalities may range from Tetralogy of Fallot to patent ductus arteriosus. In addition, they may have gastrointestinal, skin, and nervous system malformations.
Causes of Edwards syndrome
The origin of the genetic alterations lies in an error during the division of the gametocytes, either in the eggs or in the spermatozoa. That is, the gametocytes will have an altered number of chromosomes, both in excess and in deficiency. Thus, the product of conception will have an altered genetic load.
Edwards’ syndrome is caused by this type of error in cell division. Almost always by nondisjunction in one of the gametocytes; a whole, extra chromosome 18 is found in all cells of the body.
But it can also occur by phenomena such as mosaicism, in which some cells have an extra chromosome, while others have a normal genetic load. Partial nondisjunction is another possible cause of trisomy 18.
Researchers have not yet determined the specific cause of the syndrome. According to the Spanish Association of Pediatrics, duplication of the 18q12-21 and 18q23 regions is necessary for it to occur. In addition, high maternal age increases the probability.
You may be interested in: What Are Genetic Markers and What Are They For?
Diagnosis and treatment
Gynecological appointments are essential for the prenatal diagnosis of the disorder. A simple ultrasound may show an enlarged uterus and an excessive amount of amniotic fluid. In addition, the placenta may be smaller at birth.
Once the baby is born, the various physical signs and symptoms of the disease, as well as malformations, will be observed. However, the clinical manifestations can be similar to those of Down syndrome, so it’s important to make a differential diagnosis with a chromosome study.
The chromosome study will allow a detailed observation of each and every chromosome, and the additional 18 can be noted. Unfortunately, there’s no specific treatment and only complications such as cardiovascular and gastrointestinal alterations can be treated.
Prognosis of Edwards syndrome
Unfortunately, mortality in children with Edwards’ syndrome is high, due to the number of associated malformations. This fact was demonstrated in a publication by The Pan Africa Medical Journal. In addition, survival in the first year of life is negligible, with only 1 in 10 newborns making it through this stage.
In the most extreme cases, children don’t make it past the first week of life. There are a small number of cases in which children reach adolescence, however, they have serious health problems and a significant delay in psychomotor development.
A serious pathology that has no cure
Edwards syndrome is one of the most common genetic alterations, after Down syndrome. The condition causes multiple severe, life-threatening malformations.
Although there’s no effective treatment, it’s possible to make an intrauterine diagnosis. This will allow parents to make certain decisions before birth, always under the guidance of a trusted specialist.
All cited sources were thoroughly reviewed by our team to ensure their quality, reliability, currency, and validity. The bibliography of this article was considered reliable and of academic or scientific accuracy.
- Rosa RF, Rosa RC, Zen PR, Graziadio C, Paskulin GA. Trisomy 18: review of the clinical, etiologic, prognostic, and ethical aspects. Rev Paul Pediatr. 2013 Jan-Mar;31(1):111-20.
- Kepple JW, Fishler KP, Peeples ES. Surveillance guidelines for children with trisomy 18. Am J Med Genet A. 2021 Apr;185(4):1294-1303.
- López-Ríos V, Grajales-Marín E, Gómez-Zambrano V, Barrios-Arroyave F. Prolonged survival in Edwards syndrome with congenital heart disease: a case report and literature review. Medwave. 2020;20(08):e8015.
- Crawford D, Dearmun A. Edwards’ syndrome. Nurs Child Young People. 2016 Dec 8;28(10):17.
- Outtaleb FZ, Errahli R, Imelloul N, Jabrane G et al. Trisomy 18 or postnatal Edward´s syndrome: descriptive study conducted at the University Hospital Center of Casablanca and literature review. Pan Afr Med J. 2020 Dec 3;37:309.
- Saldarriaga W, Rengifo-Miranda H, Ramírez-Cheyne J. Síndrome de trisomía 18. Reporte de un caso clínico. Rev Chil Pediatr. 2016 Mar-Apr;87(2):129-36.
This text is provided for informational purposes only and does not replace consultation with a professional. If in doubt, consult your specialist.







